Risk Factors of HIV among Voluntary Counseling and Testing Centers Clients, Elgenina Town, West Darfur, Sudan.
Abstract
This study was conducted in two (VCTs) at Elgenina town, the capital of West Darfur State in Sudan in period from November 2010 to February 2011, the study included all people attending VCTs in Elgeniena town for voluntary checking one hundred and fifty clients who visited the (VCT) centers and volunteered were included in this study, nonprobability sample, 150 volunteers was taken and covered all ages, One ml of blood was taken from each of the study sample and tested by rapid Immune Chromatographic (ICT) for HIV, a structured questionnaire was designed and the interviewed after a written consent to participate in the study was signed, data was analyzed using the SPSS statistical programmer and for possible association between study variables, the Chi square test was used, the study showed that 35 volunteers (23.33%) were positives, of whom 54.3% 19 were males. People having more than one sex partner were high 63.6% with statistically significant factor of getting infection (P.value = 0.00). Also, practicing unsafe sex were 5.2% another major risky (P.value = 0.00). Among the HIV positive cases 34.3% were drug users, compared to 20.9% from the HIV negatives (p. value = 0.10). There is no relation between education level and infection with HIV (p .value = 0.154). Forty two percent of the participants were single, 30% married, 10% divorced, 7.3% widows and 10.7% were separate
Author Contributions
Academic Editor: Bechan Sharma, Professor of Biochemistry & Nodal Officer: Intellectual Property Rights Cell, Chairman: Core Committee-Environmental Science, University of Allahabad, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Ahmed, M. Hussein, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
As the Acquired Immune Deficiency Syndrome (AIDS) epidemic enters the third decade, the spread of HIV is still at a frightening pace. Globally, about 14,000 new infections were reported daily in 2005. A total of 33.2 million (30.6 million – 36.1millionestemated) people are living with HIV in 2007. This figure includes the estimated 2.5 million (1.4 million – 3.6 million) adults and 0,42million (0.32 – 0.54 million) children under 15 years who were newly infected with HIV in 2007 1. Study conducted in Sudan the main result is. Most of the respondents were knowledgeable about the true transmission modes for AIDS virus very few respondents knew someone infected with AIDS (4.5%), died of AIDS (8.1%), accepted to live with someone infected with AIDS (4.7%) or to work with someone infected with AIDS (2.1%). Regarding sexual behavior, 96.5% had reported their first sexual experience between 20 and 30 years, with 85.7% reporting one or two partners, and only 1.8% reported using condom. Multivariate logistic regression showed that circumcision, religion, marital status, age at first sex, number of sexual partners, education level, and misconception of knowledge are the main risk factors associated with HIV/AIDS 2. The proportion of women living with HIV in Latin America, Asia and Eastern Europe are slowly growing, as HIV is transmitted to the female partner of men who are infected. In Eastern Europe and Central Asia, it is estimated that women accounted for 26 per cent of adults with HIV 1. In Sub – Saharan Africa 17.7 million (15.1million 20.9 million) women are living with HIV, and for every ten adult men living with HIV there are about 14 adult women who are infected with the virus Sub-Saharan Africa is the most world’s adversely affected region. It was estimated that approximately 22.5 million people were living with HIV, and approximately 1.6 million AIDS-related deaths occurred, and approximately 1.7 million people were newly infected with HIV in 2007, of the 22.5 million 20.9 million– 24.3 million, the total number of people living with the virus. Unlike other regions, the majority of people living with HIV in sub-Saharan Africa (61%) are women. The estimated number of deaths due to AIDS in 2007 was 2.1 million 1.9–2.4 million worldwide, of which 76% occurred in sub-Saharan Africa 3. In Sudan, according to Sudan National HIV/AIDS Program (SNAP) the prevalence rate ranging from 0.5% for soldiers, 1% for antenatal care attendees, truck drivers, and Internally Displaced Persons (IDPs), 2.5% among female tea sellers and 4.4% among female sex workers 4. The overall prevalence rate in the Sudan according to wikipedia.org in is 1.1% According to the recent epidemiological and behavioral review on the HIV situation in Sudan 5. The overall HIV prevalence is estimated at 1.1% (0.67% in the North), however it is expected to gradually increase up to 2.2% in 2015 (1.2% for North). Data from the estimation and projection for this reporting period for the North Sudan showed that in 2009, the total number of adults and children living with HIV is about 122,216; AIDS orphans (ages 0 - 17) currently living (27,888); adults deaths, 6,301 (4,771 adults and 1530 children). The number of new HIV infections is 23,766 (21,416 adults; 2,351 children). Need for ART adult (15+) 18,423, children 2,981, while mothers needing PMTCT is estimated at 6, 715 6. These factors pose a greater risk for the already conflict displaced populations who are already characterized by poverty and low access to basic amenities such as health care, education, and income generating activities 4. HIV prevalence rates in 2009 were less than 0.1% in Egypt and Tunisia, 0.1% in Morocco and Algeria, 0.7% in Mauritania, and 1.1% in Sudan 5. Mode of transmission: The causative virus is transmitted from person to person, most frequently through sexual activity 1. The basic modes of transmission are, Sexual Contact, HIV spreads most commonly by sexual contact with an infected partner. The virus enters the body through the lining of the vagina, vulva, penis, rectum, or mouth during sexual activity. Blood Contamination, HIV may also be spread through contact with infected blood. However, due to the screening of blood for evidence of HIV infection, the risk of acquiring HIV from blood transfusions is extremely low. Needles, HIV are frequently spread by sharing needles, syringes, or drug use equipment with someone who is infected with the virus. Transmission from patient to healthcare worker, or vice-versa through accidental mistakes with contaminated needles or other medical instruments is rare. Mother infant, HIV may pass from an infected mother to her fetus, through the placenta or to her infant during delivery or by breast-feeding 7. Sexual contact, injection drug use, male to-male sexual contact and injection drug use, or heterosexual contact decreased 8. Easy bruising, Bouts of extreme exhaustion, unexplained body rashes, appearance of purplish lesions on the skin or inside mouth, sudden unexplained weight loss, chronic diarrhea lasting for a month or more 6. HIV infection continues to spread rapidly across many areas of the world among IDUs and their nondrug-using sex partners. CDC now estimates that 1.1 million adults and adolescents (prevalence rate: 447.8 per 100,000 population) were living with diagnosed or undiagnosed HIV infection in the United States at the end of 2006 9. The first case of HIV in Sudan was discovered in 1986. He was a refugee who came from Juba to Khartoum for treatment of his chronic illness. According to Sudan National AIDS Control Program, most of AIDS cases (92%) lay within the age group of 15 – 39 years. And 96% of AIDS cases were transmitted through heterosexual means, less than 1%through blood transfusion and about 3.1%mother to infant 10. Overall HIV prevalence is still low in Darfur. It is estimated that the number of IDPs who are infected are believed to be increasing in number due to increases in number of returnees from neighboring country like Chad, peace keepers from countries with high prevalence cases such as Kenya, Nigeria, Uganda and South Africa, these factors pose a greater risk for the already conflict displaced populations, which is already characterized by poverty and low access to basic amenities such as health care, education, and income generating activities 4. Early diagnosis of HIV through voluntary counseling and testing has been recognized by the World Health Organization as a major tool to reduce HIV mortality and spread. Voluntary counseling and testing (VCT) has been defined as a patient or client initiated counseling and testing in which patients undergo confidential counseling to enable an individual to make an informed choice learning his or her HIV status and to take appropriate action 4.
Material and Methods
This descriptive institution based study was conducted to study HIV status among clients attending Voluntary Counseling and Testing (VCT) centers it’s included all people attending VCTs in Elgeniena town for voluntary checking during study period between Nov 2010 to Feb 2011.
Study area Elgeniena town is the capital of West Darfur State in Western Sudan. It is a border state that occupies about 79000 km2, bounded from the North, South and East by the North and South Darfur states and from the West it shares a very long border with two African countries, Chad and the Republic of Central Africa.
Sample Size
All clients attending Voluntary Counseling and Testing (VCT) centers in Elgeniena town during study period Nov2010 to Feb 2011 were included in the study.
Data Collection
The data was collected between November 2010 up to February 2011 from the clients attending Voluntary Counseling Testing (VCT) Centers through interviews by using standard Questionnaire covering information on age, gender, socio-economic status and risky behavioral factors . Blood sample had been taken from clients for HIV test.
Data Analysis
The data was analyzed by using (SPSS) software and Chi-square x² to compare categorical data. The level of significance was taken at 0.05.
Ethical Clearance
Ethical permission for the study was obtained prior data implementation, by consulting and receiving approval from, Algenina locality, Community Leaders, and consent those who are interviewed and examined after explanation to each individual the aims of study and confidentiality of its result.
Result
The Table 1 shows the male is high 55.3% than female the study population represent 55.3%. The age group 15 up to 24 years was 39.3%,
Table 1. Show the Socio demographic profile of clients attending Voluntary Counseling Testing (VCT) centers N=150| Variable | Frequency | Percent | |
| Sex | Male | 83 | 55.3 |
| Female | 67 | 44.7 | |
| Below 15 | 8 | 5.3 | |
| Age | 15-24 | 59 | 39.3 |
| 25 – 49 | 73 | 48.7 | |
| 50+ | 10 | 6.7 | |
| Married | 45 | 30 | |
| Marital status | Divorced | 15 | 10 |
| Widows | 11 | 7.3 | |
| Separated | 16 | 10.7 | |
| Single | 63 | 42 | |
Table 2 shows that 24% of the clients attending Voluntary Counseling Testing were drug users.
Table 2. illustrate substance abuse among clients attending Voluntary Counseling Testing (VCT) centers| Drugs use | Frequency | Percent | |
| Valid | yes | 36 | 24 |
| no | 114 | 76 | |
| Total | 150 | 100 | |
Above Table 3 show substance used among clients attending Voluntary Counseling Testing alcohol drinking represents 16.7 %, followed by inhalation, smoking 3.3%, 0.7% was IVD, and the 76% (114) were found not to be using any substance.
Table 3. shows types of substance abuse among clients attending Voluntary Counseling Testing (VCT) centers| Types of drugs | Frequency | Percent | |
| Valid | Alcohol drinking | 25 | 16.7 |
| Smoking | 5 | 3.3 | |
| Inhalation | 5 | 3.3 | |
| IVD | 1 | 0.7 | |
| not applicable | 114 | 76 | |
| Total | 150 | 100 | |
Above Table 4 show female more affected than male23.9% and 22.9% male.
(Table 5)
Table 4. Illustrate the relationship between HIV/AIDS infection and gender among clients attending Voluntary Counseling Testing (VCT) centers N=150| Variable | Positive | Negative | Total | ||
| Gender | Male | Count | 19 | 64 | 83 |
| % | 22.90% | 77.11% | 55.30% | ||
| Female | Count | 16 | 51 | 67 | |
| % | 23.90% | 76.10% | 44.70% | ||
| Total | Count | 35 | 115 | 150 | |
| % of Total | 23.30% | 76.70% | 100.00% | ||
| Age | Variable | Positive | Negative | Total | |
| Below 15 Year | Count | 1 | 7 | 8 | |
| % | 12.50% | 87.50% | 5.30% | ||
| 15-24 Year | Count | 15 | 44 | 59 | |
| % | 25.40% | 74.60% | 39.30% | ||
| 25-49 Year | Count | 17 | 56 | 73 | |
| % | 23.30% | 76.70% | 48.70% | ||
| 50+ Year | Count | 2 | 8 | 10 | |
| % | 20% | 80% | 6.70% | ||
| Total | Count | 35 | 115 | 150 | |
| % of Total | 23.30% | 76.70% | 100.00% |
The above Table 6 show there is no relation btween monthly income and HIV/AIDS infection
Table 6. show relationship between monthly income levels and HIV/AIDS infection among clients attending Voluntary Counseling Testing (VCT) centers N=150| Income | Monthly income SDG | Positive | Negative | Total | |
| Less than 300 SDG | Count | 21 | 60 | 81 | |
| % | 14.80% | 74.00% | 54.00% | ||
| 300-600 SDG | Count | 10 | 36 | 46 | |
| % | 21.70% | 78.30% | 30.70% | ||
| 600+ SDG | Count | 4 | 19 | 23 | |
| % | 17.40% | 82.60% | 15.30% | ||
| Total | Count | 35 | 115 | 150 | |
| % of Total | 23.30% | 76.70% | 100.00% | ||
The above Table 7 show there is strong relation btween practicing unsafe sex and HIV/AIDS infection
Table 7. Illustrate the relationship between practicing unsafe sex and HIV/AIDS infection among clients attending Voluntary Counseling Testing (VCT) centers ,N=150| Variable | Result | |||
| Positive | Negative | Total | ||
| Practicing unsafe sex | No | 4 | 73 | 77 |
| % | 5.20% | 94.80% | 51.30% | |
| Yes | 31 | 42 | 73 | |
| % | 42.50% | 57.50% | 48.70% | |
| Total | Count | 35 | 115 | 150 |
| % of Total | 23.30% | 76.70% | 100.00% | |
The above Table 8 show there is strong relation between number of six partners and HIV/AIDS infection. (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6)
Table 8. show relationship between number of six partners and HIV/AIDS infection among clients attending Voluntary Counseling Testing (VCT) centers N=150| Variable | Result | |||
| Positive | Negative | Total | ||
| Number | One Person | 7 | 4 | 11 |
| % | 63,6% | 36,4% | 7,33% | |
| More than one | 20 | 18 | 38 | |
| % | 52,6% | 47,4% | 25,33 | |
| Not practicing | 8 | 93 | 101 | |
| % | 7,9% | 92,1% | 67,33% | |
| Total | Count | 35 | 115 | 150 |
| % of Total | 23.30% | 76.70% | 100.00% | |
Figure 1.The length of the period of practicing sex among clients attending Voluntary Counseling Testing (VCT). N=150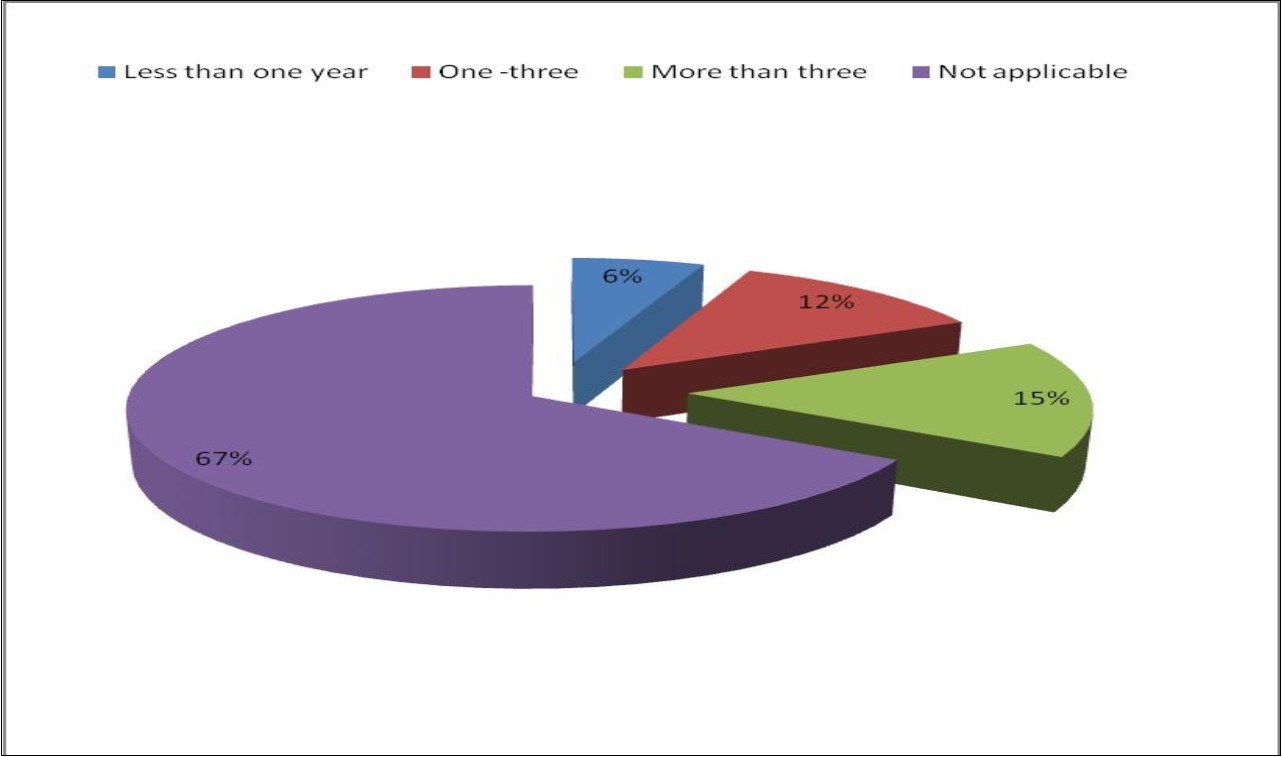
Figure 2.Reasons behind practicing sex among respondents attending Voluntary Counseling Testing (VCT). N=150
Figure 3.Frequency of use of condoms among respondents at the Voluntary Counseling Testing (VCT). N=150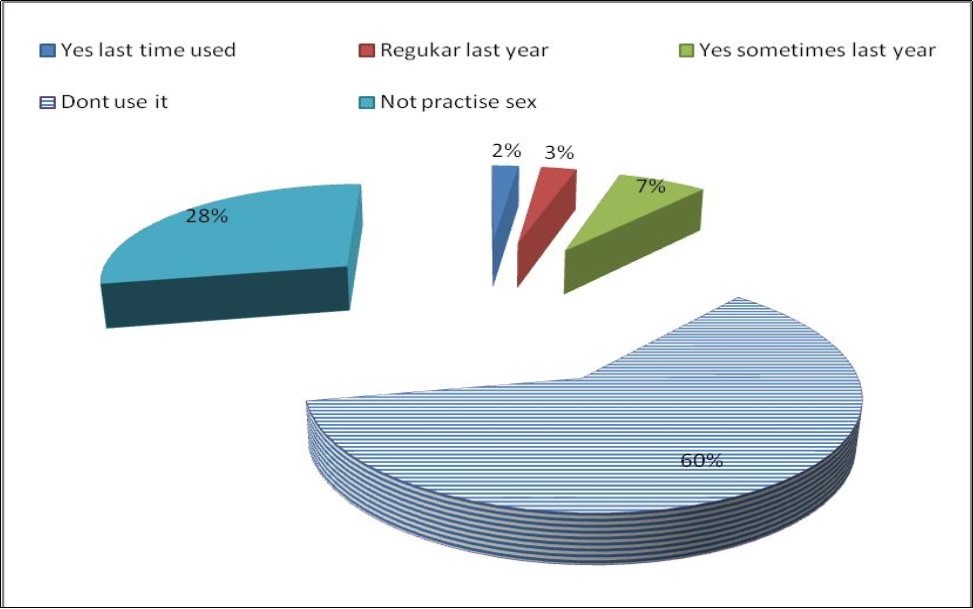
Figure 4.Occupation of clients attending Voluntary Counseling Testing (VCT). N=150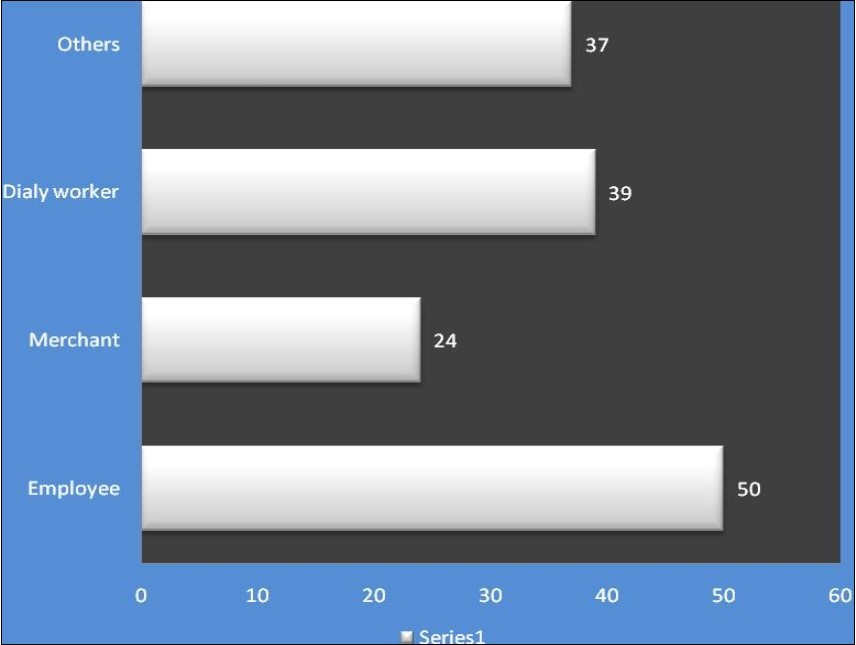
Figure 5.Reasons behind practicing sex among clients attending Voluntary Counseling Testing (VCT) centers. N=150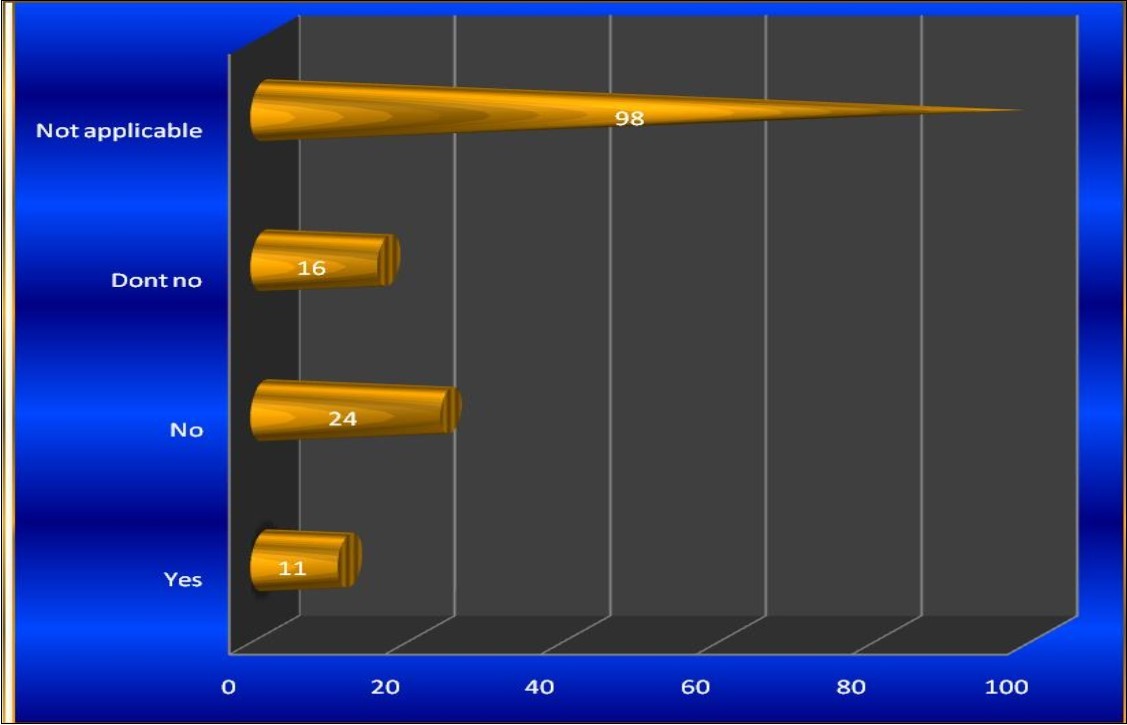
Figure 6.The main source of hearing about HIV/AIDS among clients attending Voluntary Counseling Testing (VCT) centers. N=150
Discussion
The study showed that there was no significant difference between gender and getting HIV/AIDS infection this result is similar to that mentioned by (Park’s, 2009.) “HIV/AIDS affects men; women and children in all parts of the World”, there is no significant relation between education levels and becoming infected this finding disagrees with what was announced by AIDS Behav. (2007) “Study on association between education attainment and HIV infection showed that the HIV prevalence rate decrease significantly with each increase in education attainment for both men and women, also a cohort study in rural Uganda showed a significant association between higher educational attainment and lower” and this may be due to that the disease is behavioral more than educational. also there was a strong relation between number of sex partners and infection (P. value = 0.00) (around 52.6% of the infected client have more than one partners). This finding is corresponding to what was mentioned by Park (2009) “certain sexual practice increase the risk of infection more than others, e.g., multiple sexual partners, anal intercourse, and male homosexuality .higher rate of HIV infection is found in prostitutes”. there is a strong relation between practicing of the unsafe sex and getting infection (P. value = 0.00) (about 43.1 % of infected clients are practicing unsafe sex). This agrees with what was announced by UNAIDS (2010), the vast majority of people in sub-Saharan Africa continue to be infected with HIV through unprotected heterosexual intercourse and onward transmission of HIV to infants”.
Conclusion
The proportion of infection is similar in those who attained highest level of education and those who attained low level of education. Unprotected sex and multi partners are the major risk behaviors. Clients aged between 25 – 49 represent highest infections rate 17% followed by clients aged 15 – 24 with infection rate 10%.
Acknowledgment
I would like to express my profound thanks and to acknowledge to those who helped me to conduct this study and write up the report. My special thank is due to my supervisor Dr. kamil Mirghani Ali, the dean of Faculty of Public and Environmental Health for his greater support and guidance during all steps of this study. Also I am indebted to HIV/AIDS control program department Ministry of Health- West Darfur state for their support and help. Finally my thanks go to everyone who made effort to help me finalize this study.
References
- 2.Badreldin Abdelrhman Mohamed, Mohamed Salih Mahfouz. (2013) . Factors Associated with HIV/AIDS in Sudan BioMed Research International Volume 2013, Article ID 971203, 6 pages.
- 3.UNAIDS global update on HIV report (2010) epidemic update and health sector progress towards Universal Access.
- 4.. Help Age international Organization (2009)HIV/AIDS KAP Survey among Young & Older People in West Darfur , Sudan .
- 8.CentersforDisease Control and Prevention (2014).HIV Surveillance Report,vol.24. http://www.cdc.gov/hiv/library/reports/surveillance/.PublishedNovemberAccessed [date] DiagnosesofHIVInfection intheUnited StatesandDependentAreas.
- 9.. Centers for Disease Control and Prevention.(2008) HIV Surveillance http://www.cdc.gov /hiv/library/reports/surveillance .