
Massive Left Atrium from Severe Mitral Stenosis due to Rheumatic Heart Disease: Clinical Images Not Usually Seen in Modern Radiology and Ultrasound
Abstract
Rheumatic heart disease is becoming far less common in the developed world, and therefore expsoure to its complications are been seen less by clinicians. With the increasing ease of world travel, patients with less commonly seen medical conditions are increasingly presenting to Hospitals requiring management of their complications. We present a case of an elderly lady who was a tourist in Australia, who presented with complications of her rheumatic heart disease, and her subsequent radiological and echocardiographic investigations were a significant surpirse for her treating clinicians.
Author Contributions
Academic Editor: Anil TOMBAK, Faculty of Medicine, Turkey.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2019 Andrew S Lane, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
We present a case of a small 64-year-old woman with examination findings and investigations consistent with severe mitral stenosis. Only with further investigation by transthoracic echocardiography (TTE) did the extent of the left atrial dilation become evident.
Aims
This case demonstrates the extent to which the body can compensate leading to significant alterations of anatomical structures. It also highlights the importance of clinical acumen, integrating history and examination along with multi-modal imaging into the management of the critically ill patient.
Case Presentation
A 64-year-old woman was admitted to the Intensive Care Unit (ICU) after a medical emergency team (MET) call from the cardiology ward due to a reduced level of consciousness and respiratory distress. Past medical history included rheumatic fever as a child and chronic atrial fibrillation. She had been admitted to hospital 3 days previously with worsening shortness of breath. On observation she was drowsy but rousable to voice, with a respiratory rate of thirty breaths per minute. Examination revealed a raised jugular venous pressure, a pan-systolic murmur as well as a long mid-diastolic murmur, both loudest at the apex and radiating to the axilla, a soft first heart sound, a displaced tapping apex beat, and bi-basal medium-intensity inspiratory crepitations. Her electrocardiogram showed atrial fibrillation with a rapid ventricular response of 126 beats per minute. Her arterial blood gas demonstrated an acute on chronic respiratory acidosis with a pH 7.02, PaCO2 176 mmHg, and a HCO3- of 43 mmol/L. An antero-posterior (AP) chest x-ray on admission displayed cardiomegaly, splayed carina and hilar venous congestion, with a lateral film showing the left atrium occupying a significant part of the chest cavity (see Figure 1a, Figure 1b).
Figure 1a.Chest X-ray Antero-posterior view. Findings showing enlarged left atrium, splaying of the carina, hilar venous congestion
Figure 1b.Chest X-ray Lateral view. Findings showing enlarged left atrium occupying large amounts of the thoracic cavity, both horizontally and vertically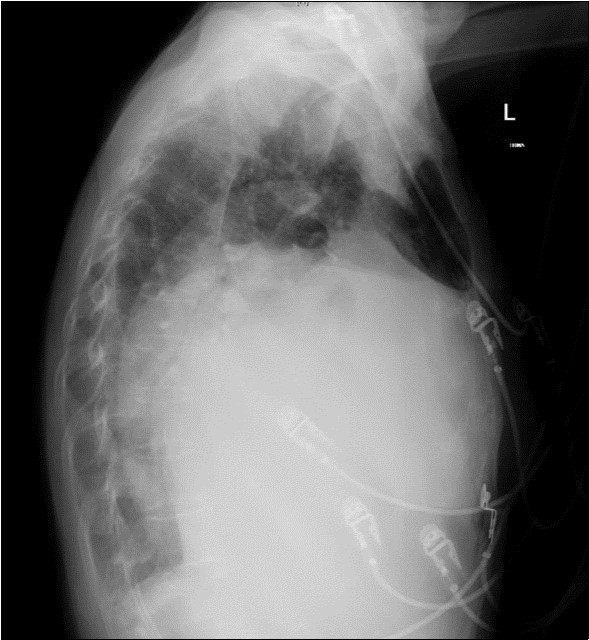
A dramatically dilated left atrium was seen on a TTE (see Figure 2a, Figure 2b, Figure 2c, and Figure 2d). Severe mitral stenosis with associated regurgitation was evident, with a mean gradient across the valve of 11mmHg and a hyperdynamic left ventricle. The left atrial volume measured by Simpson’s biplane method (see Figure 2c) was 2108mL, or 1548.5 ml/m2, based on height 1.55 metres and weight 44 Kg. Normal left atrial volume in a woman is 16 - 34 ml/m21. The computed tomography scan (CT) chest AP view (see Figure 3) is also shown.
Figure 2a.Transthoracic echocardiogram Apical 4C view. Findings include severely enlarged left atrium, severe mitral stenosis with associated regurgitation, a mean gradient across the valve of 11mmHg with a hyperdynamic left ventricle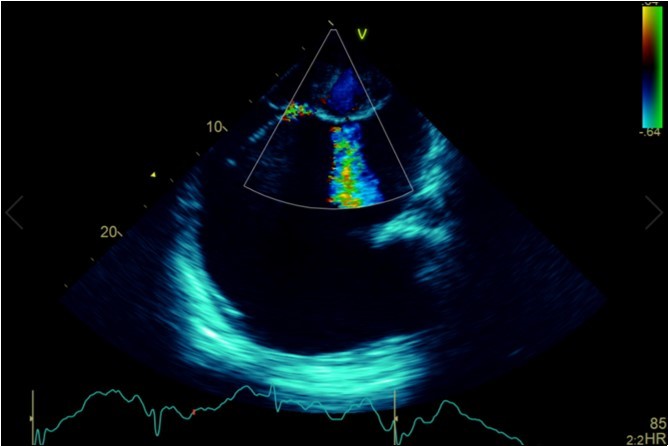
Figure 2b.Transthoracic echocardiogram Parasternal long axis view. Findings include severe mitral stenosis (‘hockey-stick’ appearance to mitral valves), raised left atrial pressure (interatrial septum fixed and bowed to right)
Figure 2c.Transthoracic echocardiogram Apical 4C view. Left atrial size estimation by Simpson’s biplane method from apical 4C view.
Figure 2d.Transthoracic echocardiogram Apical 2C view. Left atrial size estimation by Simpson’s biplane method from apical 2C view. Severely enlarged left atrium (estimated 2108ml, 1548.5ml/m2)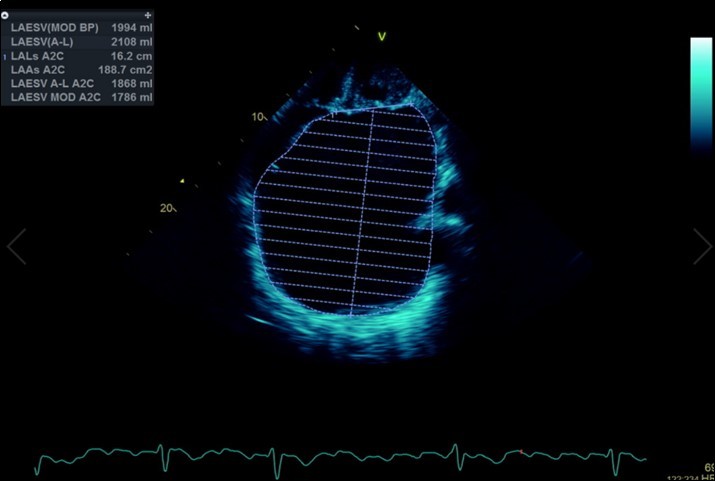
Figure 3.Computed tomography scan (CT) chest AP view, showing the extent of the left atrium filling the left and right hemithoraces.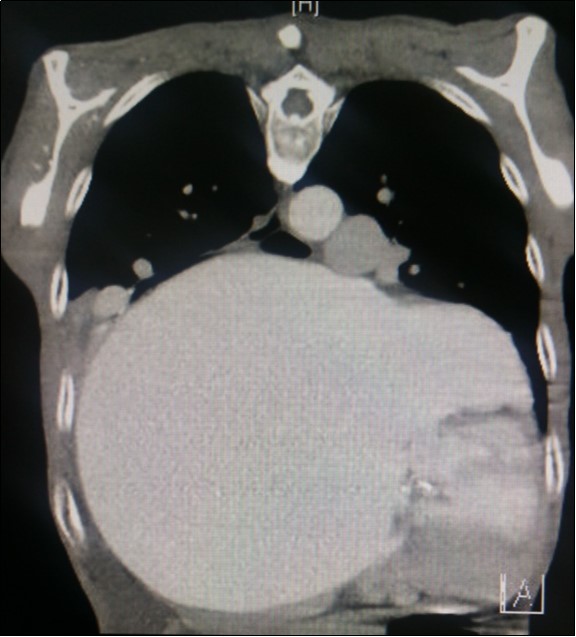
Massive left atrial dilatation is a recognized phenomenon in chronic mitral stenosis, and is considered by some to be protective against the development of pulmonary oedema in mitral regurgitation 2. Left atrial dilatation to this extent is not usually seen in living patients, however. The largest described left atrium was 3000 ml at autopsy, with another measuring 1760 ml at autopsy in 19313. Other reports in living patients include a left atrium that was estimated at approximately 2000ml on magnetic resonance imaging 4.The more precise measurements for the left atrial size we recorded on cardiac ultrasound have not been described previously. Considering the size of the left atrium, it is surprising that the mean gradient across the mitral valve was only 11mmHg. Although this is certainly severe, it could be expected that a gradient would be higher based on the severity of the left atrial dilation. We hypothesize that the gradient may have been greater previously, however the massive dilation of the left atrium may have subsequently led to a dilation of the mitral annulus, leading to an improvement in the mitral valve effective orifice area, and hence a reduction in the severity of the mean mitral valve gradient.
Our patient was an overseas visitor who had previously refused an offer of cardiac surgery. She improved clinically with two days of non-invasive ventilation and diuresis, and was discharged to the cardiology unit for ongoing medical management. It was likely that without surgery her prognosis would have been poor as she would have been at significant risk of further and cardiorespiratory compromise. One month later she successfully underwent surgery, and subsequently returned overseas after an uncomplicated post-operative recovery.
Conclusions
This case is a timely reminder that due to the ease of international travel for elderly patients, medical conditions that are rarely seen in developed countries may still present to clinicians. Modern imaging techniques rarely depict alterations of anatomy to this extent, and emphasizes the ability of the human body to compensate for chronic pathophysiological stressors. Finally, this case highlights that whilst modern imaging techniques such as cardiac ultrasound have dramatically changed the way in which we investigate and manage complex patients, clinical examination and simple radiology are still an integral part of initial assessment and management and are also needed for diagnostic purposes.
References
- 1.Lang R M, Badano L P, Mor-Avi V, Afilalo J, Armstrong A et al. (2015) Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. , Journal of the American Society of Echocardiography,e14 28, 1-39.